Rotator cuff problems are very common. In fact they are one of the main problems I deal with in my job as a physical therapist. Rotator cuff problems come in many different names such as tendinitis, bursitis, and impingement syndrome. With this article I will describe the basic anatomy of the area and the ways it can malfunction leading to pain and how this applies to training.
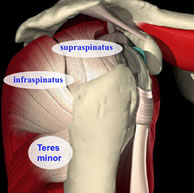
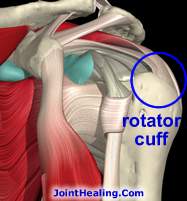
The rotator cuff is a group of four small muscles in the shoulder: the supraspinatus, infraspinatus, teres minor and subscapularis. All four muscles originate on the scapula (shoulder blade) and insert on the greater tuberosity area of the humerus (upper arm bone). The supraspinatus is the topmost muscle and the one most often involved in rotator cuff tears. The supraspinatus tendon has a delicate circulatory supply that begins to lessen in middle age, making it susceptible to injury. The subscapularis is on the anterior(front)surface of the shoulder blade. The infraspinatus and teres minor almost blend together and make up the posterior aspect of the rotator cuff.
The rotator cuff muscles as a group act to stabilize and control the glenohumeral(aka shoulder)joint. Their activity contributes to the normal active movement of the shoulder. Individually the muscles have differing actions. The supraspinatus assists the deltoid in producing elevation of the upper arm. The infraspinatus and teres minor have the same action of rotating the humerus externally, which is very crucial to normal function of the shoulder as I will explain. The subscapularis acts to rotate the humerus internally. Although there are two rotator cuff muscles producing external rotation compared to only one for internal rotation, the natural balance of strength in the shoulder favors internal rotation. Why? Because in addition to the subscapularis the pectoralis major, latissimus dorsi and teres major(all very thick, strong muscles I might add...)act to internally rotate the humerus. This imbalance sets up the potential for the development of pathology. In addition to the relavent muscles some review of the bony anatomy is helpful.
The glenohumeral joint is a "ball and socket" joint. In addition to the humerus and glenoid fossa, however, there is another very important bony structure we need to consider. This structure is called the acromion process, which is a projection of the scapula. The acromion process acts like a "roof" over the ball and socket joint. In between the "roof" and the ball and socket lie some delicate structures most notably the supraspinatus tendon. Now here's where things get interesting. Normally, when the upper arm moves into flexion or abduction(swings upward), the ball glides further down in the socket to avoid "bumping into" the "roof". Also, the humerus rotates externally to avoid the greater tuberosity ramming into the acromion.
Generally, with rotator cuff problems, something goes wrong with these delicately balanced mechanics. Things happen that allow the head of the humerus to glide upward rather than downward, and the greater tuberosity does not rotate out of the way. When this happens the delicate supraspinatus tendon gets pinched, hence the term "impingement". With repetition this will cause the tendon to become inflammed and swollen(and painful!) With the swelling the size of the subacromial space is further reduced, therefore further increasing the potential for impingement. What causes these disruptions? Well one of the most prevalent things is weakness of the rotator muscles themselves. With this weakness, the head of the humerus is not pulled down as usual. If the posterior muscles are weak, the greater tuberosity does not rotate out of the way. Sometimes the problems are due to tighness. If the powerful internally rotating muscles are tight, full external rotation is not possible and again the greater tuberosity will not rotate out of the way causing impingement. In addition, the internally rotating muscles, especially the pecs, contribute to rounded shoulders if tight. Round shoulders change the natural alignment of the shoulder blades in such a way that impingement is more likely to occur with arm movement. Sometimes the issue is structural. A certain percentage of people have what looks like a "hook" on the underside of their acromion which jabs into the supraspinatus tendon during upward movement of the arm. Imagine a little thorn jabbing into that tendon with every movement...OUCH!!! Of course many times these things occur in combination, making the problem even trickier. In addition to the above, our daily use of our arms can contribute greatly as well. People who do a lot of work at or above shoulder height are more vulnerable. As the arms are held at this height for long periods, the small muscles fatique, allowing the above alterations in mechanics to occur. Throwing athletes are at risk especially in the posterior muscles. With throwing, the arm is rapidly and forcefully internally rotated. The posterior cuff has to contract eccentrically (a "negative" in lifting terms) to slow down and stop this movement. Now if you remember the above anatomy lesson, there are only two tiny little muscles, the infraspinatus and teres minor, to counteract the forceful contraction of the pecs, lats, teres major and subscapularis. Needless to say these little muscles often get fried with constant abuse like this.
Finally, there are training considerations in the production of cuff problems. Several exercises can contribute to impingement. Included are behind the neck presses and pulldowns/chins. These exercises force a degree of external rotation that the person may not have the flexibility for. Upright rows are potentially hazardous because they involve upward movement of the humerus while it is fully internally rotated, causing the greater tuberosity to impinge against the acromion.
My suggestions for preventing this nasty problem? First off, avoid the above mentioned exercises. Second, train the little muscles: the infraspinatus and teres minor. A good way to do this is to lay on your side holding a light dumbbell in the topside arm. Bend the elbow to 90 degrees and keep it there. Now, while keeping your elbow at your side, slowly swivel your forearm upwards until the forearm is just above parallel to the floor. Generally I'd say start with three to five pounds and work the sets up to 20 reps in slow deliberate form. If you're a throwing athlete, you may want to emphasize the negative a bit, as that is how the muscles function in throwing. After paying attention to the rotator muscles I would make sure to keep the pecs and lats stretched out. Leaning through a door way with the forearms against the doorframe at about shoulder height is a common stretch given in PT. Pay attention to good posture so as to keep the scapular alignment normal. Hold your chest high, keep your head above your shoulders (think tall) and keep the shoulder blades pulled slightly down and back. Finally avoid abuse of the area functionally. Sustained or repetitive activity at or above shoulder height can promote impingement.
Whew! I haven't written this extensively since college! I hope this is informative and helpful and stimulates further ideas and questions.
"Are You Tired of Suffering From
Nagging Shoulder Pain?"
Discover How a Medically Proven Exercise Program Designed by a Physical Therapist Will Finally Allow You to Stop Relying on Medications, Injections and Other Useless Remedies to Eliminate Your Rotator Cuff Pain and Prevent Future Shoulder Injuries.
The Ultimate Rotator Cuff Training Guide provides 100% of the info you
need to resolve rotator cuff symptoms, improve strength, handle post-rehab shoulder training or safely continue working out while experiencing rotator cuff problems.
Learn how to heal your painful shoulder without ever seeing the doctor.

 The glenohumeral joint is a "ball and socket" joint. In addition to the humerus and glenoid fossa, however, there is another very important bony structure we need to consider. This structure is called the acromion process, which is a projection of the scapula. The acromion process acts like a "roof" over the ball and socket joint. In between the "roof" and the ball and socket lie some delicate structures most notably the supraspinatus tendon. Now here's where things get interesting. Normally, when the upper arm moves into flexion or abduction(swings upward), the ball glides further down in the socket to avoid "bumping into" the "roof". Also, the humerus rotates externally to avoid the greater tuberosity ramming into the acromion.
The glenohumeral joint is a "ball and socket" joint. In addition to the humerus and glenoid fossa, however, there is another very important bony structure we need to consider. This structure is called the acromion process, which is a projection of the scapula. The acromion process acts like a "roof" over the ball and socket joint. In between the "roof" and the ball and socket lie some delicate structures most notably the supraspinatus tendon. Now here's where things get interesting. Normally, when the upper arm moves into flexion or abduction(swings upward), the ball glides further down in the socket to avoid "bumping into" the "roof". Also, the humerus rotates externally to avoid the greater tuberosity ramming into the acromion.
 Finally, there are training considerations in the production of cuff problems. Several exercises can contribute to impingement. Included are behind the neck presses and pulldowns/chins. These exercises force a degree of external rotation that the person may not have the flexibility for. Upright rows are potentially hazardous because they involve upward movement of the humerus while it is fully internally rotated, causing the greater tuberosity to impinge against the acromion.
Finally, there are training considerations in the production of cuff problems. Several exercises can contribute to impingement. Included are behind the neck presses and pulldowns/chins. These exercises force a degree of external rotation that the person may not have the flexibility for. Upright rows are potentially hazardous because they involve upward movement of the humerus while it is fully internally rotated, causing the greater tuberosity to impinge against the acromion.